The ketogenic (keto) diet has gained huge popularity in recent years. Some follow it for weight loss, others for blood sugar control or overall metabolic health. Yet one key question remains:
👉 Does the rise in LDL cholesterol (often called “bad cholesterol”) seen on keto automatically mean a higher risk of heart disease?
A groundbreaking study led by Dave Feldman and Dr. Matthew Budoff (Cedars-Sinai, USA), published in 2024/2025, brings surprising answers.
🔬 Who Are Lean Mass Hyper-Responders (LMHR)?
These are people who, on a ketogenic diet, experience:
- very high LDL cholesterol (often >200 mg/dL),
- high HDL (“good cholesterol”),
- low triglycerides,
- lean body mass and excellent metabolic health.
This unique profile is called Lean Mass Hyper-Responder (LMHR). For doctors and patients alike, it raises questions, since traditional medicine links high LDL directly with heart disease.
🧪 How Was the KETO-CTA Study Done?
- 80 participants on keto for an average of 4.7 years, all with LDL ≥190 mg/dL (average ~272 mg/dL, some up to 591 mg/dL).
- 80 matched controls from the MiHeart study with typical LDL (~123 mg/dL).
- Both groups were similar in age, sex, BMI, blood pressure, and smoking history.
- Researchers used advanced imaging: coronary CT angiography (CCTA) and CAC scoring, which measure arterial plaque and calcium buildup in the heart.
📊 Key Results
- No difference in total plaque volume between the keto group and controls.
- CAC score (arterial calcium) – median = 0 in the keto group vs 1 in controls.
- No correlation between LDL levels and plaque burden, even when LDL exceeded 500 mg/dL.
👉 In other words: for LMHR individuals, high LDL did not translate into more arterial plaque in this study.
💡 What Does This Mean?
- Individual response matters – not everyone on keto reacts the same way.
- LDL is not the whole story – markers like ApoB, HDL, triglycerides, and insulin sensitivity may give a better picture of risk.
- Monitoring is key – imaging tests (CAC, CCTA) can show real cardiovascular health rather than relying only on LDL numbers.
- Short-term data – participants were on keto ~5 years. Heart disease often takes decades, so more long-term research is needed.
🦶 Why Write About This on a Foot Health Blog?
Because heart and vascular health directly affect foot health.
- Poor circulation can cause serious foot complications.
- Strong metabolic health protects not only the heart, but also the feet that carry us every day.
✅ Bottom Line
The Feldman-Budoff study suggests that for Lean Mass Hyper-Responders, very high LDL on keto may not automatically mean higher heart disease risk. Still, more long-term evidence is needed.
👉 The best approach: care for your whole health – cholesterol, blood sugar, exercise, sleep, and regular check-ups.
- Lipid Profile: Keto vs Control

Top chart: Lipid profile (LDL, HDL, Triglycerides) comparing the Keto (LMHR) group with controls.
Bottom chart: Median CAC scores – showing no meaningful difference despite very high LDL in the keto group.
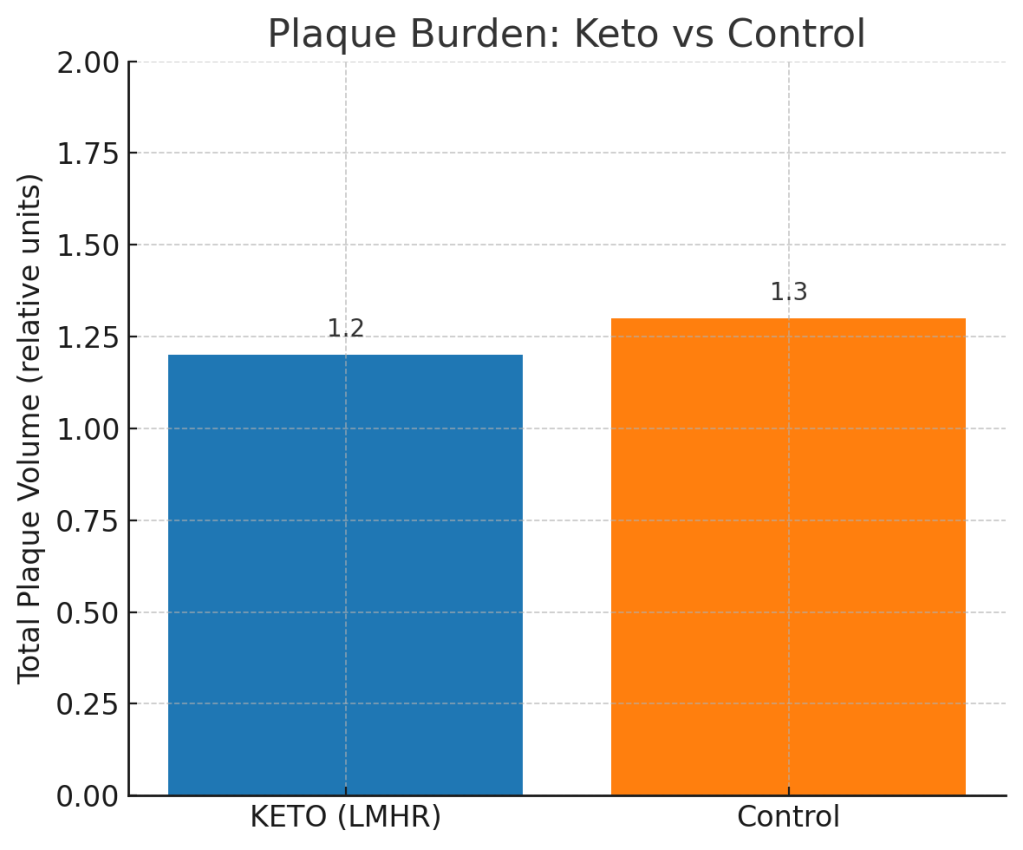
Plaque Burden: Keto vs Control
It shows that total arterial plaque volume was almost identical between the Keto (LMHR) group and the control group – matching the study’s conclusion that extremely high LDL did not translate into greater plaque.
🧪 How Was the KETO-CTA Study Done?
This was an observational, non-randomized, matched cohort study — meaning participants were not randomly assigned to diet groups.
Researchers compared 80 people who had followed a ketogenic diet for an average of 4.7 years (all with LDL ≥ 190 mg/dL, average ~272 mg/dL, some up to 591 mg/dL) with 80 matched controls from the MiHeart study who had typical LDL levels (~123 mg/dL).
Both groups were similar in age, sex, BMI, blood pressure, and smoking history.
Advanced imaging — coronary CT angiography (CCTA) and coronary artery calcium (CAC) scoring — was used to measure arterial plaque and calcium buildup in the heart.
Because this was not a randomized controlled trial, the results do not prove cause and effect, but they do provide strong observational evidence that, in this specific population, high LDL on a ketogenic diet did not correspond to more arterial plaque.
📚 Reference
Budoff, M. J., Soto-Mota, A., Norwitz, N. G., Feldman, D., et al. (2024). Carbohydrate restriction–induced elevations in LDL cholesterol and atherosclerosis in lean mass hyper-responders: The Keto-CTA study. JACC: Advances. https://doi.org/10.1016/j.jacadv.2024.101109

Leave a comment